What is Bladder Cancer
Bladder cancer is the 7th most common cancer in the male population and 11th in the general population. The disease, which is usually seen after the age of 40, is diagnosed as a result of the investigation of the complaint of bleeding in the urine. Bladder tumor can be diagnosed with ultrasound, computed tomography (CT) or magnetic resonance (MR) scans as a result of complaints such as painless clotted bleeding in the urine, burning in the urine, and frequent urination.
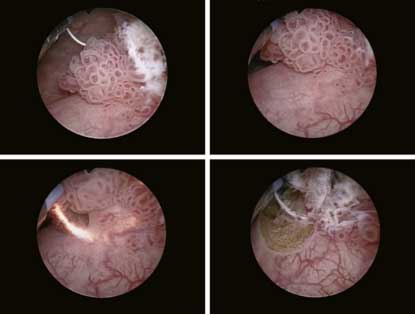
However, for a definitive diagnosis, these patients receive a clinical diagnosis together with the endoscopic procedure of the bladder, called cystoscopy, and the tumor seen during this procedure is taken into pathological examination by resection (scraping) with the help of electrocautery (TUR) or laser. The final diagnosis is bladder cancer after pathological examination.
Bladder Cancer Diagnosis
At the initial diagnosis of bladder cancer, it can be detected as local disease or disseminated disease. Local disease, on the other hand, is divided into two groups as those with spread to the bladder muscle and those without. Diseases without local and muscle spread are followed by intravesical drug administration (such as chemotherapy, immunotherapy) and intermittent bladder endoscopy for at least 5 years.
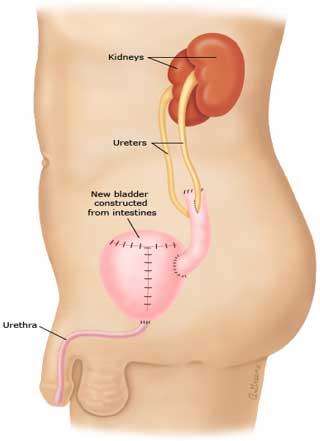
If bladder cancer with local and spread to the bladder muscle is suitable for surgery in terms of general condition, the operation of removing the bladder and making a new bladder from the bowel sections (radical cystectomy) is done.
Medical (chemotherapy) and radiation (radiotherapy) oncological treatments are applied for the disease that has spread to the bladder muscle that is not suitable for surgery and the disease that has spread throughout the body.

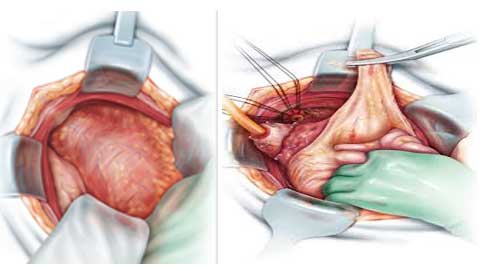
Open Radical Cystectomy
Removal of the bladder by open surgery
It is an operation performed in case of advanced stage of bladder cancer (disease that has spread to the bladder muscle and deep layers of the bladder) and if it extends to nearby organs (such as prostate, uterus, vagina).
Intestinal cleansing and oral feeding are interrupted 1-3 days before the surgery (different protocols are available). In order for patients to recover quickly in the postoperative period, short bowel protocol in our clinical routine and avoiding drugs that slow down bowel movements such as anesthetics and pain relievers (''ERAS Protocol'') provides a quick return to normal life.
In an open radical cystectomy operation performed with a 10-12 cm incision extending from the navel to the genital area, the bladder, prostate gland, seminal vesicles and lymph stations around the bladder are routinely removed in male patients. In the ureters, which are the channels where the kidneys drain urine into the bladder, all tissues are sent to pathology by cutting from the part close to the bladder. In the female patient, in addition to the bladder, uterus (womb), ovaries, tubes and upper 1/3 of the vagina, the lymph stations and the last parts of the ureters are removed and sent for pathological examination.
If there is no spread, the urethra (the last exit channel where urine travels after the bladder and prostate) is not removed in men and women. Tubes that drain urine from the kidney are usually mouthed to the skin (abdominal skin) or urethra (to the normal outlet) by using intestinal segments in order to ensure the excretion of urine from the body.
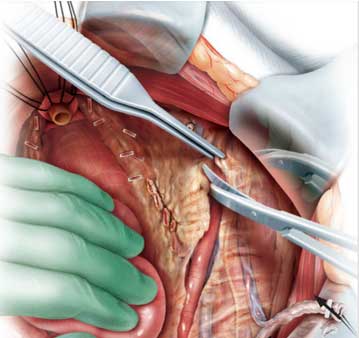
In accordance with the general systemic evaluation of the patient before the operation, physical examination, the report of the endoscopy procedure, the pathology reports, radiological examination, and if the patients are suitable during the operation, the bladder made from the intestine can be placed in its normal anatomical place as an "orthotopic bladder" and the patients can urinate from the normal outlet.

In patients who are not suitable for orthotopic bladder in the preoperative evaluation, with the ''ileal loop'' technique, which is the most widely used method in the world, the patient's urine is mouthed to the abdominal skin with a bridge made from the small intestine. This stoma, which is made permanently, is kept in a closed system with the help of urostomy bag and adapter. They empty the urine in the bag into the toilet at regular intervals.
Patients usually go out with 2 drainage systems to take out and follow the post-operative accumulations. The incision made in the abdominal region is closed aesthetically with minimal scarring. They are kept under observation in the hospital for 5-7 days in total and followed closely. In terms of the general situation after the operation, sometimes after staying in the intensive care unit for 1 day, all care and drug treatments in the inpatient service are performed in accordance with the ERAS protocol (Enhanced Recovery after Radical Surgery), and they are returned to normal life as quickly as possible.

The success of the robotic radical cystectomy operation, which usually takes 4-6 hours in total, depends on its oncological and functional results. These results are directly proportional to the experience of the surgeon and his team. According to the results of the post-operative pathology report, patients who do not require any additional treatment (radiation therapy, chemotherapy) are followed closely in terms of recurrence or distant leaps in the first 5 years.
Robotic Radical Cystectomy
Bladder removal with the help of a robot
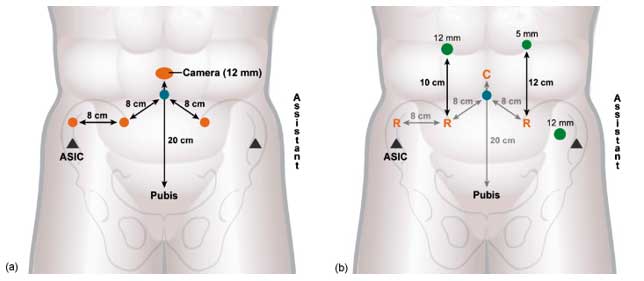
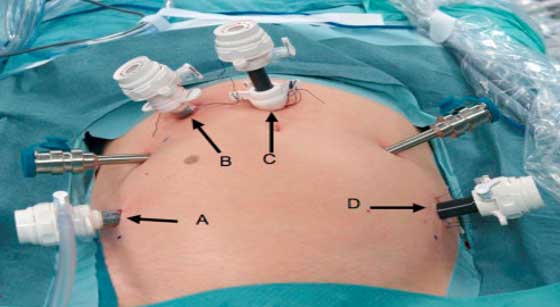
The working principle of robotic systems in urological surgery is 5-6 1 cm holes are drilled in the abdominal wall, the abdomen is inflated and the robot arms are integrated into the patient in this area. The operation is performed with a surgeon who provides remote management (console) of the integrated system and assistants helping him at the bedside. In urological cancer surgeries, robotic surgery is preferred to open methods due to its high vision quality and low amount of bleeding, and short hospitalization periods; In terms of ease of use and comfort, there is a tendency to become widespread due to its superiority over the laparoscopic (working through the holes drilled into the abdominal wall at the patient's bedside) method. The most important disadvantage is that it is more expensive than all methods in terms of cost.
Intestinal cleansing and oral feeding are interrupted 1-3 days before the surgery (different protocols are available). In order for patients to recover quickly in the postoperative period, short bowel protocol in our clinical routine and avoiding drugs that slow down bowel movements such as anesthetics and pain relievers (''ERAS Protocol'') provides a quick return to normal life.
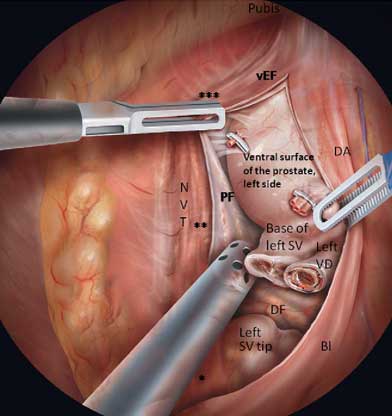
In the first part of the robotic radical cystectomy operation, the necessary tissues for treatment and staging are removed. The technique performed without any change in surgical principles in robotic radical cystectomy is different. In this operation, the bladder and its appendages (prostate, seminal sacs, lower end of the ureters in men; uterus, ovaries, tubes and part of the vagina in women) are removed with the help of a robotic system. Again in this system, the lymph stations of the bladder are removed.
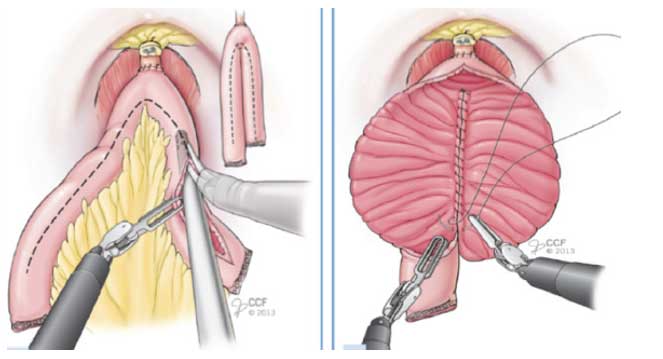
In the second part of the operation, diversion techniques, which are performed as orthotopic bladder (operation that provides urination through the normal urinary canal) or ileal loop (opening the bowel segment to the abdominal wall by using it as a bridge), can be performed both openly and closed with the robotic system. In this operation, 20-40 cm (usually small intestine) intestinal segment is separated from the intestinal wall by preserving its vessels. The remaining intestinal segments are brought closer to each other and sutured and continuity is ensured.
A new bladder can be formed by folding the intestine on itself, or it can be used as a bridge to the abdominal skin after the ureters are mouthed to this segment. The ureters (carrying channel from the kidney) are mouthed to the new bladder (orthotopic bladder) and the new bladder is combined with the urethra (the last exit tunnel of normal urine) to enable the patients to urinate anatomically. The second part of this operation can be done robotically or openly. Performing robotic surgery depends on the experience of the surgical team and the condition of the patient. The incisions made for the working channels in the abdomen are closed aesthetically in a way that leaves a minimum of scars.
Patients usually go out with 2 drainage systems to take out and follow the post-operative accumulations. They are kept under observation in the hospital for 5-7 days in total and followed closely. In terms of the general situation after the operation, sometimes after staying in the intensive care unit for 1 day, all care and drug treatments in the inpatient service are performed in accordance with the ERAS protocol (Enhanced Recovery after Radical Surgery), and they are returned to normal life as quickly as possible.

The success of the robotic radical cystectomy operation, which usually takes 4-6 hours in total, depends on its oncological and functional results. These results are directly proportional to the experience of the surgeon and his team. According to the results of the post-operative pathology report, patients who do not require any additional treatment (radiation therapy, chemotherapy) are followed closely in terms of recurrence or distant leaps in the first 5 years.